
I had a wonderful visit with my surgeon, Dr. Mel Kurtulus, this past Tuesday. It was a follow-up appointment to discuss last week’s ultrasound results and my ongoing complaints of pain and, what I suspect, is a return Endometriosis.
Due to my documented location and severity of pain, another surgery (at my request), the doc is agreeable to performing a “peek under the hood” as we like to call lit. So, the date is May 13, 2020. Surgery Number Five since my 2014 diagnosis.
What’s gonna happen depends on what he sees once he’s inside, but here’s the plan:
- Excision of any Endometriosis lesions;
- Removal of any adhesions;
- Removal of any ovarian cysts;
- Removal of the left ovary (again, at my request as this has been my Endometrioma problem-child); and,
- A routine check inside the bladder (Cystoscopy).
If, and ONLY if, it is warranted by either my insane tracking (and soon-to-be more in-depth journaling of my quality of life while suffering from any uterine cramps): the uterus and cervixes (that’s right; there’s two) may be removed. Due to the risks and complications such an addition to the above list of surgeries may pose, we’ve opted to wait until the surgery is either absolutely medically necessary by destroying my quality of life or go in and remove the uterus and cervixes at a later time. But again, he may deem the procedures medically necessary depending on what he sees once he’s inside me. Won’t know ’til the day of, but right now I’m bankin’ on I’ll have my uterus and cervixes for a while longer.
I accepted the risks and reasons we discussed in not performing the hysterectomy this May. And am super grateful he took the time to explain them all. Although, the discussion is not off the table yet; remember, if my journaling shows that it’s severely impacting my Q. of L., then it may sway the decision! Time will tell.
So, what goes on during these surgeries? I know that any EndoWarrior reading this blog knows. But what about those who haven’t gone through it? I feel like now would be an appropriate time to cover that.
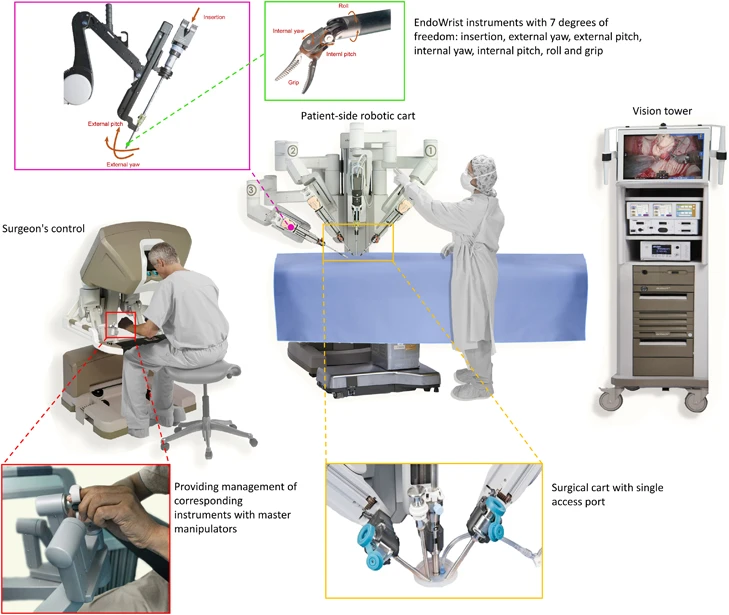
I have only ever had robotic-assisted laparoscopic surgeries for my Endometriosis. So I can only attest to my experiences. Robots? Yes. Robots. Well, one big spidery-lookin’ robot called the DaVinci. Let me preface this with I AM NOT A DOCTOR…this is purely my understanding of what has happened during my surgeries. If you’re a medical professional reading this and want to correct anything, please let me know.

Itty bitty tools are controlled by the surgeon who is sitting several feet away at a computer console with joysticks, for lack of a better word! These tiny tools can be precisely maneuvered and manipulated and the zoom-in capability of the camera is terrifying! But amazing!

So, he sits at the console. The OR staff assist with ports and moving equipment, etc. And the anesthesiologist does his own thing; they all work together to make sure I’m well cared for and not dying on the table…
Speaking of the table, I’ll be on it, tied down, covered in a drape, and put up in the not-so-typical gyno-stirrups position (aka Allen stirrups). The OR staff will likely add some tools like a uterine manipulator, a catheter, etc. Then the incisions will begin.
If history shall repeat itself (based off of 2014, 2016, July 2018, and Nov. 2018 op reports):
An small incision at the belly button allows for a small tube to be inserted into my abdomen and CO2 gas pumped in (I’ve had as much as 3 liters of gas for my surgeries). Inflate the belly! “Why?” you ask? So the gas distends the belly, shifting the organs around, and giving the surgeon a better visual of EVERYTHING going on inside. And then when the table is tipped slightly at an angle, most of the free organs shift a wee bit more, allowing greater access to the pelvic cavity.

Once proper balloony-big-belly has been achieved, a device called a trocar is placed into the incision of my belly button. Think of a trocar as a hollow tube where the camera and surgery tools can be slipped in without screwing with my incisions. More incisions to the right and left of my abdomen will be made, the number depends on what’s needed during surgery. I’ve had two, three, four, and five in the past. More trocars are placed in each incision.
A camera is inserted usually through the belly button trocar, an inspection is made and, (in my case) the Endometriosis and adhesions are visualized. I’m then tipped backwards and somewhat upside down; a position known as the Trendelenburg position. Again, this allows greater access to the pelvic cavity and the surgeon works his magic.

Is it quick? Nope. Sometimes it’s a 2-hour surgery; sometimes it’s a 4.5-hour surgery. And for others? It can be much longer…It all depends on the sheer number of lesions, the presence of adhesions, and a myriad of other factors including if there’s any organs involved, etc.
Endometriosis lesions can take a variety of shapes and colors. They may look like little freckles, or large blisters, or just stains inside the body. And the colors can range from clear, to pink, to red, to brown, to blue, to black and anything in between. It’s not an easy task, and again takes an experienced, skilled surgeon to recognize and remove the lesions.

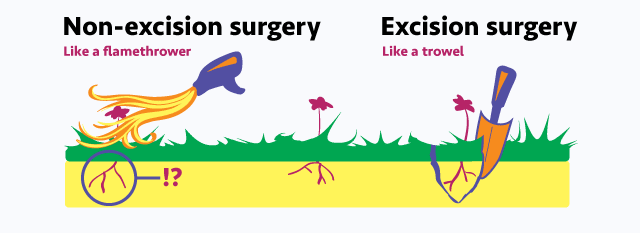
Now that they’ve spotted the Endometriosis, they go about handling it. Excision is considered the best way to remove the lesions: cutting them out. Not all surgeons practice excision. Others may just burn the lesion, which may lead to leaving the root of the lesion beneath the surface of the pelvic tissue or organs. Scarring is also more likely to occur. Excision is when they cut out the lesion in its entirety, and remove a margin of healthy tissue around it. Is it a guarantee the illness won’t come back? No. Unfortunately. Even the best-trained experts have cases of recurrence with their patients. And, if you’re reading your op report(s) and see that a heat tool or laser was used during your surgery, please don’t automatically assume it was ablation. Call your surgeon and ask. Some heat tools can be used during excision as a way to cauterize the area.
Once the surgeon has completed their task, it’s time to close you up. Equipment and materials are removed, counted, recounted, and recounted. Trocars are removed. The gas is expelled as best they can. Now this part is interesting. Trapped gas can be insanely painful during surgery recovery. It’s not like you can just fart or burp it out. The CO2 gas either 1) causes immense pain because the gas is hanging out inside the pelvic cavity (not inside the stomach or intestines like normal “gas”) or 2) the CO2 gas has damaged some nerves along the way. There’s back-and-forth debate about what causes that insane shoulder pain after a laparoscopy. But my surgeon has employed a new trick and has named it the “Lisa Special” after I asked him what he did that was so different after my second surgery. All of my girls who go to him request it. And all of them have marveled at the difference compared to other surgeries they’ve had.
The Lisa Special: Before that last incision is closed, he has the anesthesiologist inflate and deflate the lungs a few extra times…like deep breaths…and it helps push out a lot of the remaining gas that’s hiding along the nooks and crannies of the pelvic cavity. He told me once that he even heard the gas escaping from the incision. I hope it sounded much like a farting balloon.
And then? The incisions are closed and the recovery process begins. Endo excision is not an easy ordeal. It’s not simple. It’s not easy. And the recovery and healing take a lot of time. And it can be painful.
For me, my minimal recovery time off of work is two weeks. Sometimes I wish I had three weeks. But the restrictions aren’t lifted for a few more weeks after that. No bending, no squatting, no pushing, no pulling. I can’t lift anything heavier than a half-gallon of milk. No driving for the first two weeks. It’s intense. And let’s not even discuss the pain of the recovery itself, or the shoulder pain if there’s any CO2 gas left, or the agony of not being able to get comfortable to sleep, or the need to get up and take tiny walks around the house every few hours.
And the hardest part? Watching friends and family go through it with you. The fear, anxiety, nervousness, pain, and heartache. But we’re all in this together. And I’m super grateful to those who help me during my recovery time. Fewer things are more degrading than not being able to get out of bed, sit on the toilet, or even walk around the house without someone there to help.
I’m ready for this surgery. And I’m not. I find myself dwelling on “I can’t believe I’m having another one…” and “What if he doesn’t find anything?” And those thoughts put in my a quiet, introspective, sad mood.
My husband reminded me last night that I say “What if he doesn’t find anything” before every surgery. And every time, he does find more Endometriosis and scar tissue. So I need to remind myself that I know my body, I recognize this pain, and something is wrong.
Even if he doesn’t find Endometriosis, he’ll find something.
I hope.
I’m using up all of my vacation and sick days for my recovery. So he’d better find something
PS – A few of my EndoWarriors and I have decided to name my left ovary since it’s coming out: “Ophelia”…aka “I feel ya”. Another EndoWarrior (you know who you are, Stalker) I know has suggested a bon voyage party for Ophelia. We’ll see how I feel closer to May…but I’m amenable to the idea. Now? To revisit the “Tips and Tricks” before and after surgery and buy a new muumuu!
**
~ Again, I am a layman. I do not hold any college degrees, nor mastery of knowledge. Please take what I say with a grain of salt. If curious, do your own research. Validate my writings. Or challenge them. And ALWAYS feel free to consult with your physician. Always. Yours ~ Lisa


I am so sorry that you have to have another surgery and that you sure still in pain. I will be sending you healing thoughts starting now till after the surgery. Hugs to you my Warrior Sister!
LikeLike