

I have heard from several EndoWarriors that they suffer from leg pain; whether it be their hips, upper thighs, or radiating pain down their leg(s). Today we delve a bit deeper into leg pain complaints and Endo. Have upper leg pain? Lower back pain? Tailbone pain? So do a lot of people…but so do a LOT of women with Endometriosis. A 2011 study surveyed 94 people with Endometriosis. Of them, 51% complained of leg pain. Cysts may also be contributing to leg and lower back pain. And although you may have some of these symptoms and think you have sciatic Endometriosis…please be aware that it is considered incredibly rare. And it may just be that your symptoms are a result of pelvic floor muscles being too tight (pelvic floor therapy may help) OR that adhesions and/or Endometriosis has pulled your anatomy out of whack. But, please, do read on:
Back in 1966, a study was published of two women who complained of leg pain and partial paralysis:
A 35-year-old woman had bilateral buttcheek pain, which extended down her thigh, her leg, and into her ankle. At first, her physicians suggested bursitis and advised her to keep a pain journal, especially with the weather changes. Others suspected she had a damaged disc in her back. It was because of her pain journal that she realized her symptoms occurred around her period. Her OB/GYN suspected Endometriosis and put her on Mestranol, a synthetic estrogen…which made her symptoms far worse and present every day. A week before her scheduled surgery, she could no longer extend her right foot without causing severe pain up her thigh and into her buttcheek. She couldn’t walk without crutches. She also had increased complaints of weakness. Her imaging studies were normal, but her electromygram suggested denervation in her right peroneal nerve. She also had muscle atrophy on her right side. Her uterus was found to be enlarged (as if she were 6-week’s pregnant) and a mass was detected. Upon exploratory surgery, her sciatic nerve was discolored (bluish tint) and the nerve sheath was cut “releasing a black fluid.” (Gross) The biopsy showed endometrial glands and she was diagnosed with Endometriosis of her sciatica. She also had a hysterectomy, removed both of her ovaries, and her appendix was removed. She did not have Endometriosis anywhere inside her pelvic region. A year later, she had no complaints of pain.
A 43-year-old woman complained of left leg and buttcheek pain for the past seven years. The pain worsened over the years, which extended down her left thigh, leg, and into her foot. She felt pins and needles over the top of her foot. Her pain was constant and dull, but worsened around her period. She saw her OB/GYN, who performed a hysterectomy. Her pain, however, continued to return once a month, around the time she *would* have continued to have her period. Two years later, a diagnostic imaging found a “defect” along her lumbar/sacral spine. No disc protrusion was noted, but she now complained of stiffness in her left hip and had begun to walk with a limp. A year later, she had numbness on the top of her foot and left leg, as well as muscle atrophy of her left calf. A tumor was found and removed from her spine and was diagnosed as a neurofibroma. Ten months later, she went in for an exploratory surgery of her sciatic nerve. It, too, was “infiltrated…with firm dark tissue.” Biopsy revealed Endometriosis. She subsequently had both of her ovaries removed. Three years later, she was still pain-free, but the numbness and weakness in her left leg continued.
In the ’90s, a study followed women with Endometriosis who suffered from upper leg pain, weakness, and loss of sensory control during their periods. Physical therapy didn’t help and neither did anti-inflammatories. Hormonal therapy helped a lot of the women, but not all. Where hormone treatment failed, excision surgery was performed. Although pain and loss of control diminished with hormonal treatment and surgery, the leg weakness wasn’t helped for many women. This suggested neuropathy or radiculopathy damage (aka nerve damage).
In 2007, a study of a 37-year-old woman was published. She’d been hospitalized in the past for fevers, left lower quadrant tenderness, left lower extremity pain with trouble walking, and weakness. Her previous treatments resulted in antibiotics, which helped her fever subside, but her tenderness and pain persisted. An MRI revealed cystic lesions (likely Endometriosis) and the presence of an Endometrioma. After her second hospitalization and run on antibiotics, she underwent a laparoscopic surgery. They found and excised Endometriosis lesions, as well as the Endometrioma. But the Endometrioma extended into her obturator nerve, which they cleaned up and removed the Endometrioma and all traces of foreign tissue. Two weeks after her surgery, she reported no pelvic pain and no leg pain. She was also able to walk without issue.
A study published in 2010 was about a woman with Endometriosis who complained of sciatic pain. She underwent a treatment called magnetic resonance neurography (which all insurance companies may not cover). It’s a type of MRI, but modified to focus on the nerves. This MRN found some issues with her sciatic nerve and she underwent an exploratory surgery. They located and removed Endometriosis from her sciatic notch, as well as treated her nerves so they would temporarily stop sending pain signals. After surgery, she received GnRH treatment (I’m guessing Lupron), and had significant improvements in her pain and symptoms.
A 2011 study reviewed the literature of cases from 2004 to 2010. Two hundred thirteen women complained of sciatic or glute pain for unknown reasons. They underwent exploratory laparoscopic surgeries and *lo and behold* many of them had Endometriosis on the sciatic nerve (27 patients) and deep infiltrating Endo on the sacral plexus (148 patients). Others were found to have sacral plexus vascular entrapment (37 patients) and Pyriformis syndrome (1 patient). The authors of the study suggest physicians consider Endometriosis of the sacral and sciatic regions in women who complain of pelvic and back pain.
A 2012 Letter to the Editors was published in the Journal of Neurology. It highlights the case of a 45-year-old woman who suffered from lower back pain and leg stiffness. An MRI showed possible Endometriosis on her iliac muscles and right gluteus muscles. A previous EMG, spinal MRI, CT, and PET scans came back normal. Muscle relaxers and NSAIDs did nothing to help the pain. She had no prior diagnosis of Endometriosis; however, her CA-125 levels came back high (a possible indicator of Endometriosis). She began a treatment of Lupron Depot and 3 months later reported a decrease and symptoms and another MRI showed a decrease in the amount of lesions.
A study in 2013 found that out of 30 women who complained of upper leg pain and had Endometriosis, 9 of them suffered from neuropathy. Out of the 30 women in the control group who had leg pain, but did not have Endometriosis…zero of them tested positive for neuropathy. The authors suggest that tissue biopsy and neurological examination be considered forms of diagnostic treatment in women have Endometriosis and complain of leg pain.
An October 2016 published article in World Neurology was about a 39-year-old gymnast who had complained of sciatica and back pain. She had undergone a spinal fusion at her L4/5 & L5/S1 vertebra, but it did not help with her pain. Two years later, her gynocologist suspected Endometriosis due to her monthly pain and suggested a surgery. She refused, but started Lupron Depot, which made her symptoms feel better. However, she quit Lupron Depot since she couldn’t deal with the side effects any longer and opted for a hysterectomy. Her symptoms completely resolved after a hysterectomy and removal of her ovaries, and she received a confirmed diagnosis of Endometriosis. Her spinal surgery was considered unnecessary had her physicians only known about her Endometriosis diagnosis.
A study published in the April 2017 edition of the Journal of Minimally Invasive Gynecology followed-up with women who had undergone resections of their sciatic nerves due to Endometriosis. Of them, all the women had stated that their pain had drastically reduced since their surgeries, and all had regained their gait (although for some it took up many years after surgery and therapy). So, there is hope that a sense of normalcy may be achieved with care.
In November of 2018, the Journal of Anesthesia and Perioperative Medicine published an article discussing several cases of Endometriosis-induced sciatica. Symptoms mimic that of sciatica and it is estimated that 40% of women with Endometriosis suffer from leg pain.
The documented cases of Endometriosis on or inside the sciatic nerve sheath go on and on and on. It is well-proven that it can exist there, and can cause radiating pain down the leg(s) with or without numbness, tingling, and partial paralysis.
But is all leg and lower back pain caused by Endometriosis lesions? No, some of it can be nerve damage. Leg pain and these other symptoms can also be caused by other nerve impingement or disc damage. Some women even have issues with Endometriosis in their psoas major muscle, which can affect the lower back and hips.
Studies have found that it is important to test the nerves for neuropathic pain, rather than referred pain. What’s the difference? Referred pain is pain in the body that’s not at that source (like your leg hurts, but your leg isn’t hurt). Neuropathic pain is a chronic pain condition caused by nerve and tissue damage. These damaged nerves send pain signals to wrong areas of the body…like the legs.
Some women incur neuropathic nerve damage from pelvic surgery, mostly in the following areas of the body…but these same areas can be affected by Endometriosis (as you’ve read above):
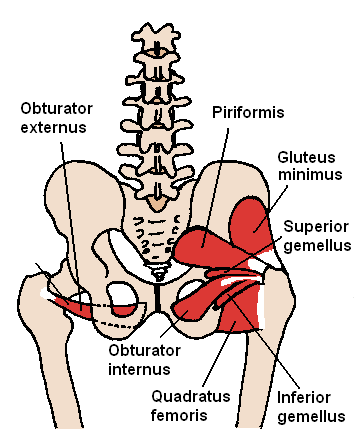
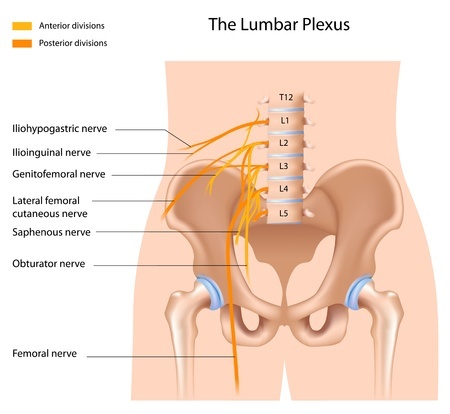
- obturator – nerves from the pelvis to the leg;
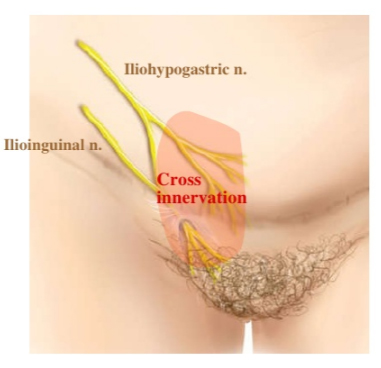
- ilioinguinal/iliohypogastric – nerves from your lumbar spine that travels down the upper and mid-thigh, and (with women) also covers our mons pubis and labia majora;
- genitofemoral – a nerve that travels to the upper thigh and mons pubis;
- femoral – the nerve that runs down the upper thigh and inner leg
- lumbosacral nerve plexus – a whole bundle of nerves that consist of the above-referenced nerves, and then some.
The post-op damage may have been the result of surgical trauma, an injury by stretching, suture entrapment, or may have been caused by the retractors used during surgery. Physical therapy or surgical repair may help reduce any symptoms of post-operative nerve damage. A 1966 study found that 36 women and 14 cadavers who had hysterectomies were found to have femoral neuropathy, likely due to the force of the retractors used during the surgeries.
What have I learned today?
Some women find relief from leg pain pain with GnRH agonist treatments, such as Lupron Depot. Others find relief after surgical intervention.
If you have pain/numbess/weakness down your leg, into your foot and ankle, on your upper thigh, around your backside, or even in your tailbone and think it may be related to your Endometriosis, have a conversation with your doctor. Or it could be nerve damage from prior surgeries. Or it could be both. Either way, talk.
If your imaging studies turn out normal, don’t lose heart. If your physician tells you that the pain is all in your head because your scans are normal or nerve block injections aren’t working, feel free to INSIST it is not.
The only way to truly diagnose if Endometriosis is impeding our sciatic or other nerves is through an exploratory surgery and biopsy of any tissues discovered. If you have a surgery pending (or would like to schedule one) and suffer from these symptoms, ask your surgeon to take a close look at your sciatic sheath, obturator nerve, or other nerves that may be affected.
Treatments range from hormone therapy, physical therapy, nerve blocks, and surgery.
Have you been diagnosed with Endometriosis that affected your sciatic nerve, obturator nerve, or legs? We’d love to hear from you. You can share your experience and I’ll publish it on our blog.
**Updated April 2, 2019**
Resources:
Clinical Imaging – (Abstract; March 1990) MRI Findings of Sciatic Endometriosis
European Journal of Obstetrics & Gynecology and Reproductive Biology (Abstract; Aug. 2014) Severity of Cyclic Leg Pain in Women with Endometriosis and in Controls – Effect of Laparoscopic Surgery
Fertility and Sterility – (Abstract; Feb. 2011) Laparoscopic Therapy for Endometriosis and Vascular Entrapment of Sacral Plexus
Fertility and Sterility – (Abstract; June 2010) Magnetic Resonance Neurography for the Diagnosis of Extrapelvic Sciatic Endometriosis
Fertility and Sterility – (Abstract; Oct. 1999) Phantom Endometriosis of the Sciatic Nerve
Fertility and Sterility – (Abstract; July 2013) Pain in the Upper Anterior-Lateral Part of the Thigh in Women Affected by Endometriosis: Study of Sensitive Neuropathy
Journal of Anesthesia & Perioperative Medicine – (Article; Nov. 2018) Chronic Sciatica Induced by Endometriosis
Journal of Bodywork and Movement Therapies – (Abstract; July 2011) A Pilot Study of the Prevalence of Leg Pain Among Women with Endometriosis
Journal of Minimally Invasive Gynecology – (Abstract; Nov./Dec. 2007) Laparoscopic Excision of Endometriosis of the Obturator Nerve: A Case Report
Journal of Minimally Invasive Gynecology – (Abstract; April 2017) Five-Year Follow-up After Laparoscopic Large Nerve Resection for Deep Infiltrating Sciatic Nerve Endometriosis
Journal of Neurology – (Article; July 2012) Sciatic Endometriosis Presenting as Period (Catamenial) Sciatic Radiculopthy
Journal of Neurosurgery – (Abstract; May 1998) Catamenial Mononeuropathy and Radiculopathy: A Treatable Neuropathic Disorder
Journal of Neurosurgery – (Abstract; Feb. 2011) Cyclic Sciatica from Extrapelvic Endometriosis Affecting the Sciatic Nerve: Case Report
Journal of Neurosurgery – (Abstract; Dec. 1966) – Endometriosis Within the Sheath of the Sciatic Nerve; Report of Two Patients with Progressive Paralysis
Journal of Spinal Disorders & Techniques – (Abstract; Oct. 2011) Cyclic Sciatica in a Patient with Deep Monolateral Endometriosis Infiltrating the Right Sciatic Nerve
Obstetrics & Gynecology – (Abstract; Aug. 2002) Postoperative Neuropathies After Major Pelvic Surgery
The Journal of the American Medical Association – (Abstract; Feb. 1966) Femoral Neuropathy – A Neurological Complication of Hysterectomy
Women’s Health Magazine – (Article; Feb. 2018) 6 Signs You’ve Got an Ovarian Cyst That’s About To Become A Problem
World Neurology – (Abstract, Oct. 2016) Cyclic Sciatica and Back Pain Responds to Treatment of Underlying Endometriosis: Case Illustration
~ Again, I am a layman. I do not hold any college degrees, nor mastery of knowledge. Please take what I say with a grain of salt. If curious, do your own research Validate my writings. Or challenge them. And ALWAYS feel free to consult with your physician. Always. Yours ~ Lisa


I think this had actually happened to me! I’ve been struggling with both severe endo and moderate fibro with a big challenge to know which was causing which symptoms. I’ve been having leg pain for years, sometimes severe enough I couldn’t walk. I had low back pain, hip pain, foot pain. Poor circulation. I was afraid I had some neuropathy. After my second excision surgery and removal of gigantic ovarian cysts, I immediately had relief from some of this pain. My legs and feet felt better! I wondered if it was all in my head and asked the doctor at post-op. He said it absolutely could be real and showed me a photo of my iliopsoaz muscle. He said the endo was attaching to that muscle and others in my pelvis, but had been removed. On top of the direct effects, the swelling and irritation in there couldn’t have been helpful. Anyway, I’m feeling dramatically better in my legs and feet so far and am anxious to see how good I’ll feel once I’m all recovered from surgery. I really think it was having major effects to my lower extremities!
LikeLiked by 1 person
Yaaaaay to feeling better!!!!!
LikeLike
This is a really interesting article. I hadn’t associated my own leg pain with Endo before. I think I’ll be having a little chat with my own GP now. Thank you!
LikeLiked by 1 person
I’ve been researching sciatic endo all day now, as a possible hypothesis for my current issues. Everything I find is just more and more (possible) validation, when taking my prior medical history into account. I had severe pelvic endo for ages. Took 14 years to diagnose. Two surgeries, and an expert hysterectomy and excision later, I had begun to hope I was one of the lucky ones. But I’ve had severe back pain issues that all routine tests are failing to diagnose. It’s gotten bad enough that I’m reliant on a rollator to get around, and I can’t work. The only variable that doesn’t completely click is cyclical pain flares–but my cycle was never regular to begin with, so I can’t really even test that now that I don’t even bleed. I’m not yet sure how I feel about this possibility. On the one hand, there aren’t enough curse words for me to express my feelings about what endo has stolen from my life already. On the other… I might be fighting a possible known foe. Until I come across another possibility that seems as likely as this, I’m going with the theory that I have sciatic endo until proven otherwise.
LikeLiked by 1 person
You have my sympathies and my support!!! You k ow your own body. Keep fighting and moving ahead!! ❤
LikeLike
This is useful, thanks for the links.
LikeLiked by 1 person
You’re very welcome!
LikeLike
This information is really useful and it helps me a lot for clearing my doubts. Best of luck for your future posts. god bless you.
LikeLike
I’m so glad it was helpful! Good luck to you!
LikeLike